Using the MLA Content Map to Plan Revision
Learn how to turn the GMC MLA content map into a realistic revision plan.
Dr M Sadler
6/18/202613 min read
How to Use the MLA Content Map to Plan Your Revision
Opening the MLA content map for the first time can feel a little like being handed an index of medicine and told to get started. There are clinical areas, patient presentations, conditions, practical skills and professional responsibilities to consider. If you try to work through every entry from top to bottom, it is easy to feel overwhelmed before your revision has properly begun.
The good news is that the content map is not meant to be memorised.
It is much more useful as a planning tool: something that helps you check your coverage, identify gaps and organise your revision around the knowledge and skills expected of a newly qualified doctor.
This guide will show you how to turn the map into a realistic study plan without creating an enormous checklist that takes over your life.
Take-home messages
Make sure you are using the version of the MLA content map that applies to your assessment date.
Use the map to check the breadth of your revision rather than trying to memorise it line by line.
Plan around patient presentations as well as individual conditions.
Judge your strengths using question performance and active recall—not simply how familiar a topic feels.
Give more time to weaker, common and clinically important areas.
Spread topics across several revision sessions instead of covering each one only once.
Move gradually from topic-based practice to mixed and timed questions.
Reviewing your mistakes is more valuable than simply completing as many questions as possible.
First, check which content map applies to you
This matters particularly for students sitting the MLA during 2026.
If your assessment is taken on or before 31 August 2026, the original MLA content map remains the relevant version.
If your assessment is taken from 1 September 2026 onwards, you should use the updated content map published by the GMC.
The updated version is divided into six domains:
Areas of clinical practice
Areas of professional knowledge
Clinical and professional capabilities
Practical skills and procedures
Patient presentations
Conditions
If you are unsure which version your medical school is using, ask your assessment team rather than relying only on your expected graduation date.
The overall planning method in this guide works with either version.
What the content map is, and what it is not
The content map describes the core knowledge, skills and behaviours that may be assessed through the AKT and CPSA.
It helps create a common framework across UK medical schools, but it is not a complete textbook or a revision course. It tells you the areas you may need to understand; it does not teach you the clinical detail within each area.
It is also not a list of predicted exam questions.
Seeing a condition on the map does not mean it will necessarily appear in your particular paper. Equally, recognising the name of every listed condition does not mean you are ready to answer an applied clinical question about it.
The map works best when you use it to ask:
Have I covered the full breadth of the assessment?
Which areas am I consistently weaker in?
Can I apply my knowledge to clinical scenarios?
Am I revising patient presentations as well as named diagnoses?
Have I included professional knowledge and clinical skills?
Think of it as a map of the territory, not the journey itself.
Step 1: Create a working copy
Start by downloading the correct content map and creating a version you can annotate.
You could use:
a spreadsheet;
a document with a table;
a printed copy;
a notes app;
your question bank’s topic tracker.
The exact system does not matter. Choose something simple enough that you will actually keep it updated.
For each area, leave space to record:
your current confidence;
your latest question performance;
when you last reviewed it;
recurring mistakes;
when you plan to revisit it.
Avoid building an elaborate colour-coded system that takes longer to maintain than the revision itself, your tracker is there to help you decide what to study next, not to become another project.
Step 2: Revise by presentation as well as diagnosis
One of the most useful features of the content map is that it separates patient presentations from conditions.
In clinical practice, patients rarely arrive and announce their diagnosis. They present with chest pain, confusion, breathlessness, weakness, abdominal pain or an abnormal test result. You then need to decide:
what the likely causes are;
which dangerous possibilities must not be missed;
what information you need next;
which investigation is most appropriate;
whether the patient needs urgent treatment.
That is also how many applied-knowledge questions are constructed. When revising a condition, connect it to the presentations through which it may appear. For example, instead of studying pulmonary embolism as an isolated page of notes, connect it with:
sudden breathlessness;
pleuritic chest pain;
collapse;
haemoptysis;
hypoxia;
a swollen leg.
Then compare it with other causes of those presentations. This helps you build clinical reasoning rather than a collection of disconnected facts. This is similar to the problem-based approach used in many medical schools, but here the aim is to organise your revision around the way patients and exam questions actually present.
Step 3: Carry out an honest baseline audit
Before creating a detailed timetable, find out where you are starting from. A simple traffic-light system can work well:
Green
You can explain the topic without relying heavily on notes, answer applied questions consistently and distinguish it from similar conditions.
Amber
You understand the main ideas but become uncertain when the presentation is unusual, the options are similar or the question asks for the next step in management.
Red
The topic is unfamiliar, your knowledge is fragmented or you repeatedly make mistakes that could lead to unsafe decisions.
Not yet assessed
You have not done enough recent question practice to judge it properly, try not to rate topics based only on whether they look familiar.
Reading about heart failure several times may make the material feel comfortable, but familiarity is not the same as being able to retrieve and apply the information independently.
Use evidence wherever possible:
Can you recall the important features without looking?
Can you explain your reasoning aloud?
Can you answer questions on the topic?
Can you interpret relevant results or images?
Can you choose safe initial management?
Do you keep making the same error?
A short baseline question set across several topics is often more informative than simply guessing your confidence level.
Step 4: Decide what deserves your time first
Not every topic needs the same amount of revision, a sensible plan gives more attention to areas that are:
weak;
commonly encountered;
clinically important;
linked with emergencies or patient safety;
easy to confuse with similar conditions;
repeatedly appearing in your error log.
You can divide topics into three broad priorities.
Priority 1: weak and important
These should appear early and repeatedly in your plan. Examples might include an area where you struggle to recognise a deteriorating patient, select immediate management or distinguish between important differentials.
Priority 2: partly understood
You know the basics but need more practice applying them, these topics often improve quickly with focused questions and careful review.
Priority 3: currently secure
These still need occasional mixed practice so that they are not forgotten, but they do not require the same amount of initial study time. This is your personal planning system, not an official exam weighting, the aim is to use your limited time sensibly while still maintaining broad coverage of the content map.
Step 5: Group the map into manageable revision blocks
Working through a long alphabetical list is rarely the easiest way to build connected clinical knowledge, instead, group related material into blocks.
You might organise revision by a systems approach such as:
cardiovascular medicine;
respiratory medicine;
gastroenterology;
neurology;
endocrinology;
renal medicine;
psychiatry;
paediatrics;
obstetrics and gynaecology;
surgery;
emergency presentations;
professional knowledge.
Within each block, connect conditions with relevant presentations, investigations, practical skills and professional issues.
For a cardiovascular block, for example, you might bring together:
chest pain;
breathlessness;
palpitations;
syncope;
acute coronary syndromes;
arrhythmias;
heart failure;
valvular disease;
ECG interpretation;
immediate assessment of an unwell patient.
This produces a more clinically meaningful revision session than studying each entry in isolation.
Step 6: Build each session around active learning
A revision session should require you to retrieve, use and check your knowledge, not simply expose yourself to it again. A practical session could follow this pattern:
1. Begin with recall
Before opening your notes, write down or explain what you already know. For a condition, you might recall:
typical presentation;
important differentials;
initial investigations;
immediate management;
longer-term treatment;
complications;
reasons for urgent escalation.
This quickly reveals what is genuinely available from memory.
2. Review the gaps
Use reliable teaching resources, your medical school materials and current clinical guidance to correct what you missed or misunderstood. Keep this focused. You do not necessarily need to reread an entire chapter because you forgot one part of the management pathway.
3. Complete applied questions
Use questions that require you to make decisions in clinical scenarios. Try to explain why your chosen answer is best before revealing the explanation.
4. Review every uncertain answer
Do not limit your review to questions marked incorrect. A correct guess may reveal just as much of a knowledge gap as an incorrect answer.
5. Schedule the next review
Return to the topic after a gap rather than considering it permanently completed. A topic should become more secure across several encounters.
Step 7: Use retrieval practice
Retrieval practice simply means bringing information to mind without first looking at the answer.
Examples include:
answering question-bank questions;
using flashcards;
writing everything you can remember about a topic;
explaining a condition aloud;
drawing a management pathway from memory;
covering your notes and recalling the next step;
teaching a topic to another student.
This feels harder than rereading because it exposes uncertainty.
That difficulty is useful. Research has repeatedly found that practising retrieval can improve longer-term retention more effectively than repeated passive study [5–7]. Retrieval is most useful when you then check your answer and correct misunderstandings. The aim is not to practise remembering incorrect information.
Step 8: Spread revision over time
One long session on a topic may produce a temporary feeling of confidence, but knowledge fades when it is not revisited. Instead of studying respiratory medicine intensively for one week and then ignoring it for two months, return to it at intervals. There is no single perfect spacing schedule for every student or topic. A simple approach might be to revisit material:
later in the same week;
one or two weeks later;
again through a mixed question set;
once more closer to the assessment.
Weak topics may need shorter intervals. Secure topics can be revisited less frequently. The key principle is that each topic should reappear in your plan after some forgetting has had time to occur. Research in health-professions education supports both distributed practice, spreading learning across time, and retrieval practice as useful approaches to improving learning outcomes.[5–7]
Step 9: Begin with focused practice, then mix topics
When you first learn or revisit an area, topic-based practice is useful, it allows you to see common patterns and consolidate the underlying framework. However, the real AKT does not tell you that the next question is cardiology or endocrinology, and it presents the topics randomly. As your knowledge improves, introduce mixed questions, a sensible progression is:
Learn or revise a topic.
Complete focused questions on that topic.
Revisit it after a gap.
Mix it with related areas.
Include it in broader random tests.
Practise under timed conditions.
Mixed practice is usually more difficult because you must first identify what kind of problem you are facing, that makes it more representative of the decisions required in an applied examination. Do not move to exclusively mixed questions too early if your underlying knowledge is still very weak. Build a basic framework first, then practise recognising when and how to apply it.
Step 10: Keep an error log that is actually useful
An error log should help you change your future performance, it should not become a second textbook containing copied explanations from every question you answer. For each meaningful mistake, record:
the topic;
what the question was testing;
why you chose the wrong answer;
the correct reasoning;
what clue you missed;
what you will do differently next time.
It can help to classify mistakes.
Knowledge gap
You did not know the relevant fact, investigation or management principle.
Interpretation error
You knew the medicine but misunderstood a result, image or clinical clue.
Question-reading error
You answered a different question from the one being asked—for example, choosing the definitive investigation instead of the best initial test.
Prioritisation error
Several options were reasonable, but you did not choose the safest or most urgent next step.
Overthinking
You talked yourself away from the most likely answer because a rare alternative seemed more interesting.
Review the log each week. If the same type of mistake keeps returning, adjust how you revise rather than simply adding more questions.
A worked example: planning revision around chest pain
Suppose your content-map audit shows that chest pain is an amber area. You recognise the major diagnoses, but you struggle when several options seem plausible. Rather than writing “revise chest pain” in your timetable, break the session down.
Start with the presentation
Recall your approach to a patient with chest pain:
immediate assessment;
important history;
red flags;
examination;
initial investigations;
when urgent escalation is needed.
Connect the important conditions
Compare the features of conditions such as:
acute coronary syndrome;
pulmonary embolism;
aortic dissection;
pneumothorax;
pericarditis;
respiratory infection;
gastrointestinal causes;
musculoskeletal pain.
The aim is not merely to list them. Ask what makes each one more or less likely and what would change your immediate management.
Add investigations and interpretation
Review areas such as:
ECG interpretation;
cardiac biomarkers;
chest imaging;
observations and basic blood tests;
selecting further investigations based on the scenario.
Complete focused questions
Use a set of chest-pain or cardiovascular questions and explain your reasoning before viewing the answer.
Record recurring errors
Perhaps you repeatedly confuse the best initial investigation with the definitive test, or miss signs that the patient is unstable. That specific problem should shape your next review.
Revisit it later
Schedule chest pain to return in a mixed acute-presentations set the following week.This is how the content map becomes an active revision plan rather than a passive checklist.
A simple weekly structure
Your timetable needs to fit around placements, teaching and life outside medicine. It does not need to look impressive on paper. A realistic week might include:
Monday
Focused revision of one weaker clinical area, followed by topic-based questions.
Tuesday
A second clinical area, with a short review of Monday’s errors.
Wednesday
Professional knowledge, prescribing, ethics or communication alongside clinical revision.
Thursday
A patient-presentation session connecting several possible diagnoses.
Friday
A mixed question set covering current and previous topics.
Weekend
Review your error log, revisit selected weak areas and plan the following week. Include clinical-skills practice separately for the CPSA. Some weeks will be disrupted by placements, nights, illness or other commitments, a useful plan should be flexible enough to survive an imperfect week.
Review your plan every week
At the end of each week, ask:
What did I actually complete?
Which topics improved?
Where did I continue to struggle?
Am I revisiting older material?
Am I doing enough applied practice?
Have I neglected professional knowledge or clinical skills?
Is my plan realistic for the time available?
Move topics between red, amber and green based on evidence. A topic should not become green simply because you have read about it, It should become green when you can retrieve the knowledge and apply it reliably. Likewise, do not be discouraged when a mixed question set exposes gaps. Finding weaknesses during revision is far more useful than discovering them during the exam!
Common mistakes when using the content map
Turning every line into a separate revision session
Many entries overlap. Grouping them around systems and patient presentations usually creates a more coherent plan.
Treating the map as a list of predictions
The content map defines the broad framework of the assessment. It does not tell you exactly which questions will appear.
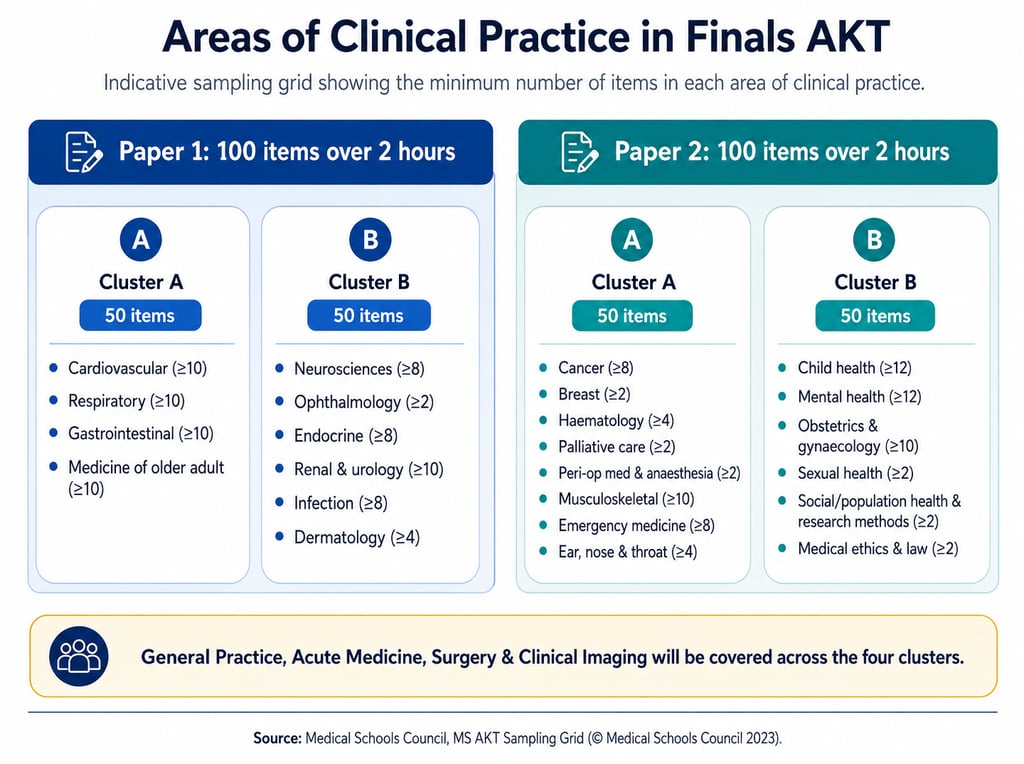
Spending equal time on everything
Your weaker and more clinically important areas will often need repeated attention. Secure areas need maintenance, not necessarily another full day of notes. MSC have published the general coverage for the MS AKT as below
Measuring progress only by questions completed
Completing 100 questions without reviewing them carefully may be less useful than completing 30 and understanding every mistake.
Revising only named conditions
Remember to include patient presentations, professional knowledge, practical skills and clinical capabilities.
Leaving mixed questions until the final week
Introduce mixed practice gradually so that recognising the topic becomes part of the challenge.
Ignoring the CPSA
The content map underpins both the AKT and CPSA. Written revision does not replace practising histories, examinations, procedures, explanations and communication.
Use official resources alongside your plan
The Medical Schools Council advises that your medical education and training provide the foundation for MLA preparation.
It also provides free official MS AKT resources, including candidate information, webinars and practice materials.[3–4]
Use the content map alongside:
teaching from your medical school;
placement experience;
official practice questions;
reliable UK clinical guidance;
a well-structured question bank;
clinical-skills practice.
You do not need to buy every revision resource available. More resources can easily lead to more organisation and less actual learning.
Choose a small number of reliable tools and use them consistently.
How ReviseMD can help
ReviseMD is designed to support both the breadth and depth of MLA revision. Its questions cover a wide range of clinical topics, mapped to every condition in the MLA content map, while detailed explanations, condition summaries, notes and personalised quizzes help you go beyond simply recognising the correct answer.
Once you have identified your stronger and weaker areas, ReviseMD can help you turn that into a revision plan that changes as your performance improves. The app highlights your Focus Areas - the topics in which you are currently scoring lowest, and gives you a quick quiz for each one. This makes it easier to decide what to revise next without repeatedly scanning the whole content map.
After completing questions, you can:
bookmark questions that you want to revisit;
add your own notes to capture the reason you made a mistake;
create custom quizzes from bookmarked questions;
build focused quizzes from questions you previously answered incorrectly;
return to weaker topics through the Focus Areas section.
This creates a useful revision loop:
Identify a weak area.
Review the underlying topic.
Complete a focused quiz.
Bookmark or annotate anything you found difficult.
Reattempt incorrect and bookmarked questions later.
Check whether the topic is improving.
Used in this way, ReviseMD becomes more than a bank of questions. It acts as a live companion to the MLA content map, helping you decide what needs attention now, what should be revisited later and which areas are beginning to move from red or amber towards green.
Final thoughts
The MLA content map can look intimidating because it shows the breadth of knowledge and capability expected at the point of graduation, you do not need to tackle it all at once. Start with the correct version, carry out an honest baseline review and group the content into manageable clinical blocks. Then combine focused learning with active recall, question practice, careful feedback and regular revisiting. Most importantly, let your performance guide your plan.
A revision timetable should not simply record what you intended to study. It should change as you learn more about your strengths, your weaker areas and the mistakes you are most likely to make. Used in that way, the content map becomes much less overwhelming. It becomes a practical guide to what you should work on next.
Related guide - What Is the UKMLA?
References
General Medical Council. Updated MLA content map: applies from September 2026.
General Medical Council. Original MLA content map: applicable to assessments taken up to and including August 2026.
Medical Schools Council. Preparing for the Applied Knowledge Test.
Medical Schools Council. Medical Licensing Assessment: frequently asked questions.
Roediger HL, Karpicke JD. Test-enhanced learning: taking memory tests improves long-term retention. Psychological Science. 2006;17(3):249–255.
Trumble E, Lodge J, Mandrusiak A, Forbes R. Systematic review of distributed practice and retrieval practice in health professions education. Advances in Health Sciences Education. 2024;29(2):689–714.
Donker SCM, Vorstenbosch MATM, Gerhardus MJT, et al. Retrieval practice and spaced learning: preventing loss of knowledge in Dutch medical sciences students in an ecologically valid setting. BMC Medical Education. 2022;22:65.
Contact
Get in touch for inquiries and support.
feedback@revisemd.uk
© 2025. All rights reserved.